FAQs about IVF terminology and procedures
What are the most common IVF terms I should know?
Some of the key terms include ovarian stimulation, egg retrieval, fertilisation, embryo transfer, and implantation. Understanding these steps can help you feel more prepared and confident during treatment.
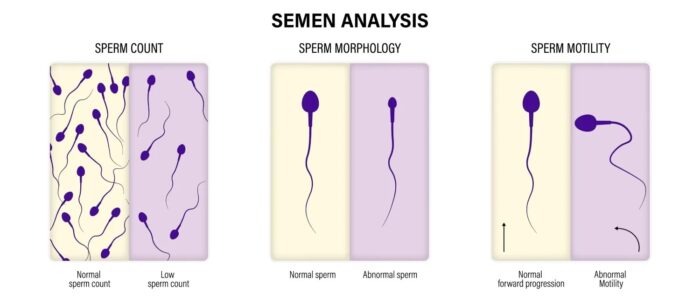
What is the difference between IVF and ICSI?
In standard IVF, eggs and sperm are mixed together and fertilisation happens naturally. In ICSI (intracytoplasmic sperm injection), a single sperm is injected directly into an egg to assist fertilisation, often used when there are male factor fertility issues.
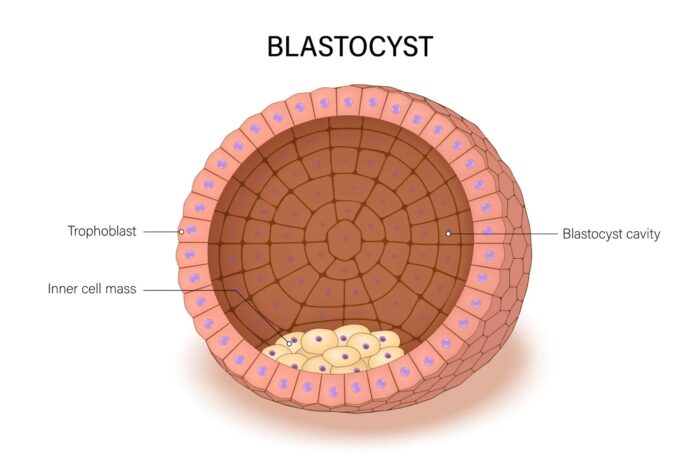
What does PGT mean in IVF?
PGT stands for preimplantation genetic testing. It involves checking embryos for chromosomal abnormalities or monogenic diseases before they are transferred to the uterus, helping to select the healthiest embryos.
How many embryos are usually transferred during IVF?
In most cases, especially for younger women or when using tested embryos or donor eggs, doctors recommend transferring one embryo to reduce the risk of multiple pregnancies. Your specialist will guide you based on your situation.
What is a frozen embryo transfer (FET)?
A frozen embryo transfer is when an embryo that was previously frozen is thawed and transferred to the uterus in a later cycle. It allows more flexibility in timing and preparation.
Can IVF guarantee a pregnancy?
Unfortunately, no fertility treatment can guarantee a pregnancy. IVF can greatly increase the chances, but success depends on factors like age, embryo quality, and overall health.
Is IVF painful?
The IVF process involves injections, monitoring, and minor procedures. Some women experience mild discomfort, but most find it manageable. Your Procriar team will support you every step of the way.
When should I consider embryo testing (PGT)?
PGT is often recommended if you are over 37 years old, have experienced recurrent miscarriages, have a known genetic condition, or have had repeated IVF failures.
How long does a full IVF cycle take?
A full IVF cycle typically takes around 6 to 8 weeks from the start of ovarian stimulation to the pregnancy test, though timings can vary slightly depending on your personalised treatment plan.
Final thoughts
Understanding IVF terminology and procedures is a powerful step toward feeling more comfortable and in control during your fertility journey.
At Procriar, we are here to guide you with knowledge, experience, and compassion. If you have any questions about IVF or would like to speak with one of our fertility specialists, please get in touch with us today. We are ready to support you every step of the way.